Chronic Inflammatory Response Syndrome (CIRS) was first used as a term in the 1990s to describe a multi-symptom, multi-system chronic illness.
Changes in cognition, hormones, and energy are commonly experienced. Exposure to certain environmental ‘inflammagens’ and pathogenic organisms (which can collectively be termed ‘biotoxins’) is understood to trigger this kind of chronic inflammatory response in the body. The work of Dr. Shoemaker showed that the toxic ‘soup’ found a water damaged building (WDB) e.g. bacteria, fungi, actinomycetes as well as tick borne infections were two of several triggers for this response.
Dr. Shoemaker’s work is intimately connected with Dr. Dale Bredesen’s work on cognitive decline and both indicate that exposure to biotoxins can be part of the pathway that leads to cognitive decline. Both Doctors also agree that resulting inflammation and eventual hypo-metabolism are the net result of exposure thereby contributing to changes in brain function. CIRS can, therefore, be seen as very much part of the cognitive decline jigsaw.
The CIRS approach has led to a broader understanding of chronic immune system activation, so whilst CIRS is not a medical diagnosis currently applicable in the UK, the concept of a chronic inflammatory response picture is something that can still be assessed and considered.
In order to assess a potential chronic inflammatory response it is important to consider what exposure you might have had e.g. exposure to a water damaged environment, a tick bite or tropical fish food poisoning. Next it is important to consider symptoms.
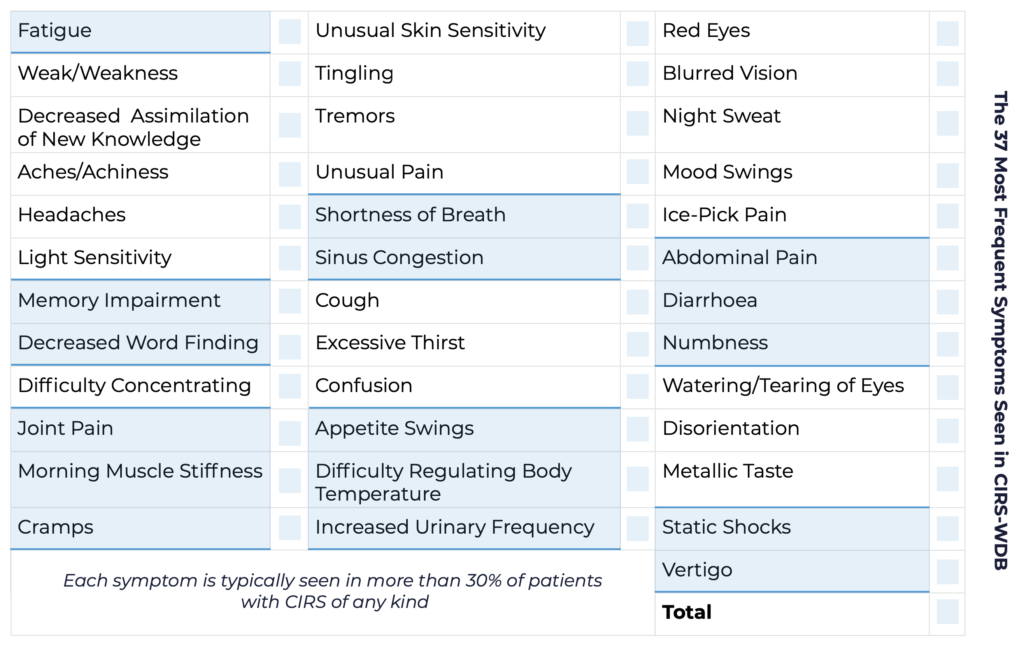
Symptoms can be varied and to some extent ‘invisible’, with neurological symptoms being common. If you think that your health may have been affected by possible exposure to any of the triggers noted above then please consider the following symptom chart. These are the 37 most frequent symptoms seen in the CIRS picture. The total score is important to note, but, each alternating colour of the chart indicates a symptom cluster. A cluster score of more than 8/13 can mean that further testing could be considered. The list given here is simply a guide and would be discussed in more detail during an appointment due to the specific nature of some of the symptom details.
Symptoms cover typical inflammation symptoms, hormone changes, neurological symptoms and respiratory tract symptoms.
It is also important to be aware that even if you have experienced exposure to a water- damaged building (or any other biotoxin exposure) and feel that your health is compromised, this may not be the only thing affecting your health. All aspects of your health will, therefore, need to be considered to get the fullest picture possible.
Testing for CIRS includes a blood test that covers inflammatory markers, hormone markers and some relevant antibodies. The nasal swab test for MARCoNS is also useful to consider especially if there are sinus symptoms, although this can still be present with no symptoms. This is relevant as hormone changes can mean there is less protection in the sinuses and so greater levels of bacterial colonisation can become more prevalent.
Where changes in cognitive health may be seen volumetric MRI testing can be important to consider.
HLA gene testing can be undertaken as can the GENIE test which reports on gene signalling, especially relating to the hypo-metabolic signature of the CIRS picture.
Finally, dust swiffer testing can be considered to check for mould/actinomycetes, mycotoxin or endotoxin exposure in an environment.
A chronic inflammatory response requires the careful consideration of a body of evidence that all builds to create a picture that is consistent with exposure. Lab test results should match symptoms and the therapeutic or treatment protocol should provide improvements that can be tracked via testing to allow for course-correction of a protocol as required.
Additional factors such as your health history, family health history, and other relevant symptoms and any prior diagnoses all have to be considered in order to give the most comprehensive understanding.
One potential protocol is the Shoemaker Protocol, this is a useful framework that utilises the lab work to guide the programme, with retesting undertaken at regular timeframes. The Bredesen protocol is also worth considering if there are cognitive symptoms, though the Shoemaker Protocol should take precedence of direction if there is a clear chronic inflammatory response picture related to biotoxin exposure.
The Shoemaker protocol is 12 steps with the first step being removal from exposure.
- Removal from exposure
- Removal of biotoxin carriage – binder prescription
- Eradication of MARCoNS
- Correct anti-gliadin antibodies/Gluten free diet/Re-check
- Correct androgens
- Correct ADH/serum osmolality dysregulation
- Correct elevated MMP9
- Correct low VEGF
- Correct elevated C3a
- Correct elevated C4a
- Correct elevated TGFb-1
- Correct VIP
Your own progress though the Protocol will depend on your initial test results and response to each step.